Stages of Birth in Heart-Centred Therapies
Diane Zimberoff, LMFT + David Hartman, LPSW
Journal of Heart-Centred Therapies, 2004, Vol. 7, No. 1
Existential Resistance to Life (excerpt)
Conception
At the time of fusion of the sperm with the egg to form a fertilized cell, the prenate may experience an eagerness to move forward with the journey into human life, or dread, or ambivalence, depending largely on the attitudes of the mother (carried in her egg) and father (carried in his sperm). If an individual feels unwelcomed or threatened by one or both of the parents, or ambivalence by either one, then surely he/she will have decidedly mixed feelings (anxiety and ambivalence) toward the unfolding journey.
There is a growing appreciation in the psychoanalytic community for the profound impact on the child of his/her parents’ feelings about becoming pregnant at the time of conception. Feder (1980) discusses the parents’ fears, ambivalence and contradictory conflicts, usually unconscious, regarding pregnancy which he terms “preconceptive ambivalence.” He suggests that the consequences of those fears and conflicts will greatly impact the future child, “whose destiny is significantly determined by both the manifest and the latent portions of the initial parental ambivalence surrounding his psychological and biological conception” (p. 164). Feder considers that, of all these preconceptive beliefs, the most damaging of all is the narcissistic hurt of realizing one is unwanted. Feder refers to the expression of this ambivalent and contradictory element in the parents’ psyche as “procreative panic,” showing up as open or covert rejection, hatred and neglect of the future child. Feder calls the absence of these ambivalent and contradictory feelings in the parents at conception, “procreative joy.” He asserts that the initial ambivalent conflicts embedded in the child even at conception continue to manifest throughout the lifespan through repetition compulsion and recapitulation.
Individuals aware of being an “unwelcome child,” e.g., parental rejection in the form of contemplated or actual adoption or contemplated or attempted abortion, react with shame and overpowering anxiety regarding their very right to exist. They may act to fulfill their perception of their parents’ desire for their death. The existential angst and death urge become deep, unconscious forces at work throughout the individual’s life. Research by Southgate and others suggests that many child accidents are in fact unconscious attempts at suicide (Southgate & Whiting, 1987).
Feldmar (1979) studied a number of adolescent patients with a history of more than five suicide attempts each, always at the same time of year. He eventually determined that the suicide dates of four patients corresponded to the month in which their mothers had tried to abort them. The adolescents had no conscious knowledge of the abortion attempts that they were unconsciously acting out. Feldmar discovered that they had even used a method of suicide similar to the method of the abortion, for example, chemicals or instruments. After discovering that their suicide attempts were seasonal intrusions of prenatal memory, the patients were free of the suicidal compulsion. They never attempted suicide again, even when their ‘anniversaries’ returned.
Implantation
Implantation is the process by which the fertilized egg attaches itself to the wall of the uterus, embedding into the uterine lining and becoming enveloped by the wall of the uterus. The individual conceptus begins questing for a suitable site to implant, one that offers fertility, nurturing and welcome. Depending on the father’s and mother’s attitudes, the individual may instead experience the uterine wall as barren, cold and toxic. Examples are (Emerson, 2002): a “narcissistic uterine wall” (quicksand that sucks one into satisfying the mother’s needs); an “entrapping uterine wall” (engulfing, full of rigid conditions and demanding expectations); or a “rejecting uterine wall” (unwelcoming, carrying the message that “I don’t really want you” or “You are a burden”). Any of these compromised sites for implantation could result in a feeling of not belonging, of confusion and ambivalence about “being here” in this life, and could activate defenses of avoidance, control or preoccupation.
Individuation
After 5 to 7 days of being completely absorbed by the mother in the uterine wall (in implantation), the conceptus begins to grow back out of the uterine wall, separating from the mother’s flesh. The separation can bring relief and a sense of freedom and accomplishment, but it can also initiate a profound sense of alienation, rejection and loneliness.
Because 60% of fertilized eggs die during implantation, and another 40% of embryos die during or after individuation, the struggle for the conceptus is one of life-or-death. In a hostile or ambivalent uterine environment, the conceptus may experience a sense of impending death, carrying a “death imprint” that contaminates the life-oriented impulse to move forward in life.
We will observe that several elements persist in experiences of avoidance, control and ambivalence in subsequent stages of development. They are feelings of rejection, confusion, foreboding, engulfment, and a sense of impending death. We find these recapitulated in later stages of prenatal life, in birth experience, and in the struggle for balance on the continuum of security/ exploration, of attachment/ individuation for infants, toddlers, children, adolescents, and adults. And there is a special connection between the conceptus’ experience of individuation and the person’s experience of death, both monumental times of separating from the mother’s (or Mother Earth’s) flesh.
Birth
The four stages of the birth experience itself, elaborated by Grof (1985) as basic perinatal matrixes (BPM), can be fertile ground for observation of the defenses against embracing life.
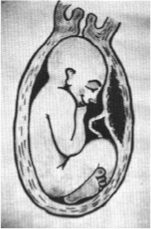
I: Intrauterine Experience
Before the Onset of Delivery
This matrix is related to the original condition of the intrauterine existence during which the child and his mother form a symbiotic unity. This symbiotic unity can be disturbed (in a toxic womb) or secure, protected and nurturing (in an optimal womb).
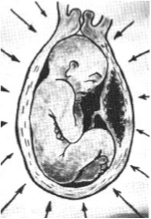
II: Contractions in a
Closed Uterine System
This episode can be one of “no exit,” especially if there is interrupted or induced labor, or ambivalence on the mother’s part. The fetus is alienated from the mother with no possibility of immediate escape which may be later manifested as feelings of being trapped and hopelessly overwhelmed.

III: Propulsion through
the Birth Canal
The uterine contractions continue, the cervix is wide open and the gradual and difficult propulsion through the birth canal begins. There is an enormous struggle for survival, crushing pressures and suffocation. The system is not closed any more, however, and an end is in sight.

IV: Separation from Mother and
Formation of a New Relationship
In this phase the agonizing experiences of labor culminates, the propulsion through the birth canal is completed and the ultimate intensification of tension and suffering is followed by a sudden relief and relaxation. Now the process of balancing attachment and individuation begins.
Obstetrical interventions in the birth process often recapitulate the neonate’s previous embrace or resistance to life. These include anesthesia, with control taken away through dissociation and thus resulting in bonding deficiencies and a desire for stimulation and contact; induced labor, with control taken away through being overpowered and thus resulting in bonding deficiencies and a desire for less stimulation and contact; forceps delivery, with control taken away forcibly, resulting in authority issues, rescue expectations, and bonding deficiencies; cesarean delivery, with mutuality in the task taken away arbitrarily, resulting in bonding deficiencies, interruption and invasion complexes, and rescue expectations. The separation of baby from mother immediately upon birth is perhaps the most damaging of interventions, as well as the most common, resulting in abandonment fears, control issues, and uncertainty about being welcome here.
